

At 6:15 a.m., the day shift board is already under pressure.
Two nurses called out overnight. A respiratory therapist is covering an extra unit. An imaging role has been open for weeks. Finance wants overtime down, but patient demand has not exactly agreed to cooperate. For hospital leaders, this is what workforce pressure looks like in real life: not one dramatic crisis, but a constant stream of staffing tradeoffs that affect care delivery, employee morale, and labor spend all at once.
That is exactly why healthcare workforce planning has moved out of the annual budgeting cycle and into day-to-day operations.
In 2026, the systems handling staffing best are not necessarily the ones with the biggest labor budgets. They are the ones that plan earlier, forecast smarter, and build a more flexible talent mix across permanent staff, float pools, allied health professionals, travel clinicians, and locum tenens providers.
Why workforce planning matters more now
Hospital staffing used to be treated as a scheduling problem. Today, it is a business resilience issue.

Healthcare leaders are managing a difficult mix of realities:
- Persistent vacancy pressure in critical clinical and support roles
- Burnout across core teams after years of sustained strain
- Growing demand tied to aging populations and more complex care needs
- Heightened pressure to control premium labor costs without sacrificing coverage
That means staffing can no longer be reactive. If an organization waits until a unit is already short, the choices usually get more expensive and more disruptive.
A stronger workforce planning strategy helps leaders answer questions before they become emergencies:
- Where are the greatest skill gaps likely to appear in the next 30, 60, or 90 days?
- Which service lines are most vulnerable to seasonal swings?
- Which roles should be filled permanently, and which are better covered flexibly?
- How much agency dependence is truly necessary, and where can it be reduced?
The shift from headcount planning to talent-mix planning
One of the biggest mistakes hospitals make is treating workforce planning as a simple headcount exercise.
A medical-surgical floor may be “fully staffed” on paper and still be operationally fragile if too many employees are new, cross-coverage is weak, or specialized allied roles are thin. The real question is not just how many people you have. It is whether you have the right mix of skills, credentials, flexibility, and coverage depth.
What that looks like in practice
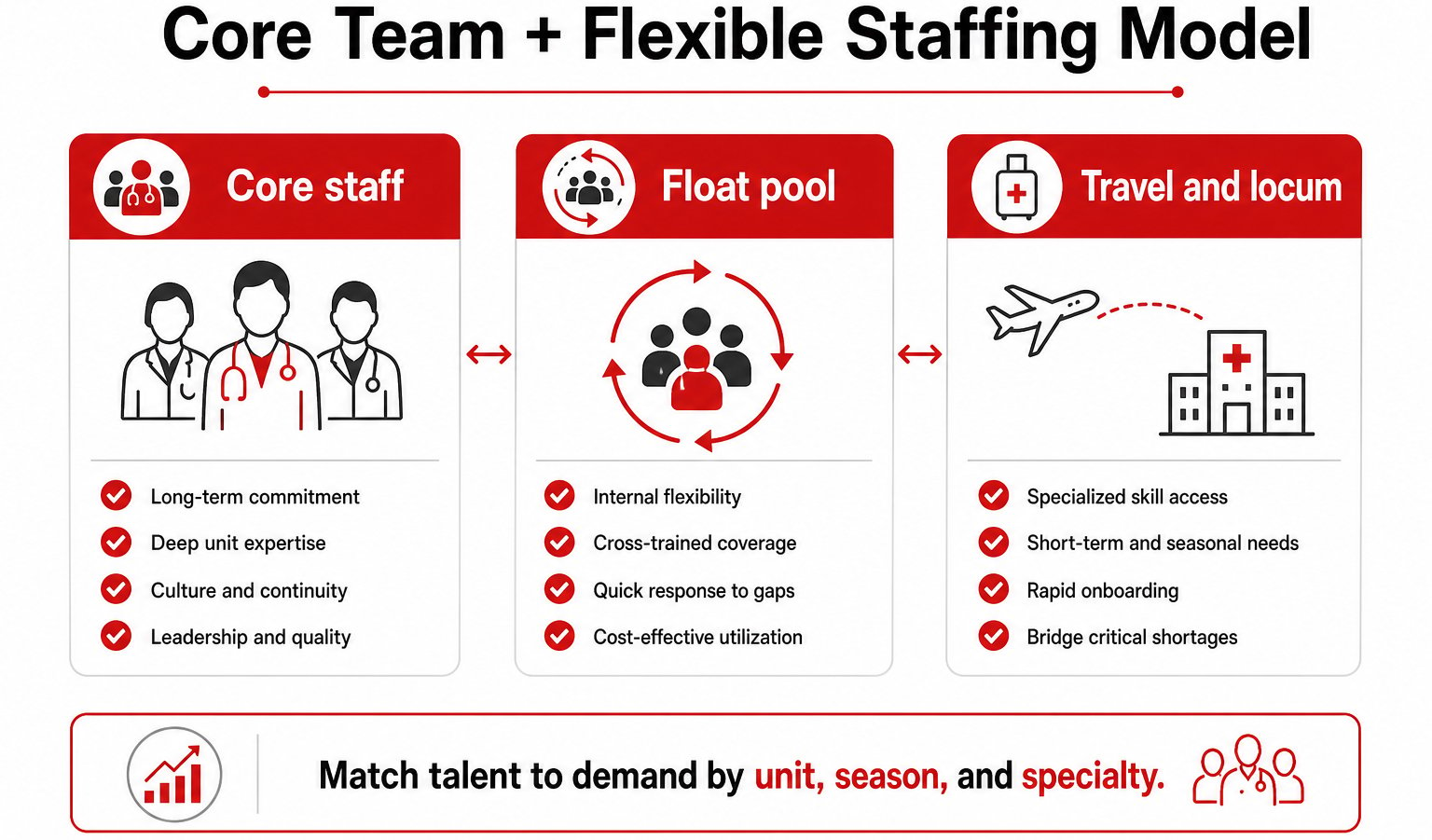
A strong hospital staffing strategy usually includes:
- Core permanent staff for continuity, culture, and patient experience
- Internal float resources for predictable coverage gaps
- Travel clinicians for temporary demand spikes or regional shortages
- Allied health staffing support for imaging, rehab, lab, respiratory, and therapy roles
- Locum tenens staffing for physician coverage, call gaps, and hard-to-fill specialties
When leaders look at staffing through that lens, they stop asking, “How do we fill every opening the same way?” and start asking, “What is the most sustainable staffing model for this service line?”
That is a much better question.
Where hospitals often get stuck
The organizations that struggle most with workforce planning are not ignoring the issue. Usually, they are trapped in one of three patterns.
1. They plan too late
By the time vacancy rates, overtime, or time-to-fill metrics start flashing red, the options are narrower. Leaders are forced into rushed contracts, coverage patches, or short-term fixes that cost more than a proactive strategy would have.
2. They focus only on nursing
Nursing is central, but it is not the whole workforce story. Allied health shortages can create just as much disruption. A delayed imaging schedule, a thin respiratory roster, or therapy bottlenecks can slow patient throughput and increase pressure on other teams.
3. They separate workforce planning from operations
The best staffing plans are built with input from clinical operations, finance, HR, and workforce partners. When those teams work in silos, staffing decisions become fragmented. A plan that looks reasonable in finance may fail on the unit floor by the second week.
A better model for 2026
Healthcare workforce planning works best when it becomes a rolling discipline instead of a once-a-year exercise.
Step 1: Forecast demand by service line
Start with actual operational patterns:
- Seasonal census shifts
- Historical callout trends
- Time-to-fill by role
- High-acuity units with fragile coverage
- Physician coverage pinch points
This helps leaders spot where demand is volatile and where coverage needs to be more elastic.
Step 2: Map critical skill gaps
Not all vacancies carry the same risk. A delayed fill in one department may be inconvenient. In another, it can affect access, revenue, or patient safety.
Prioritize roles that directly influence:
- Patient throughput
- Procedure volume
- Specialty coverage
- Weekend and night support
- Regulatory or accreditation readiness
Step 3: Build the right talent mix
This is where many hospitals unlock better outcomes. Instead of defaulting to one staffing channel, use a layered model.
For example, a hospital facing intermittent ED pressure may keep its permanent nursing base intact, strengthen float support, use travel talent during peak demand, and bring in locum coverage to stabilize physician schedules. That approach protects the core team while avoiding a scramble every time volume changes.
Step 4: Activate staffing partners strategically
The right healthcare staffing partner should do more than send resumes.
A true workforce partner helps hospitals:
- Identify high-risk roles early
- Expand access to specialized talent pools
- Fill allied health and physician gaps faster
- Improve continuity across travel, temp-to-perm, and direct hire models
- Align staffing support with labor and operational goals
That matters because speed alone is not enough. The staffing model has to support retention, patient care, and cost discipline at the same time.
Step 5: Track outcomes that matter
If workforce planning is working, leaders should see movement in more than just open requisitions.
Watch metrics such as:
- Time to fill
- Overtime hours
- Premium labor spend
- Vacancy duration by specialty
- Retention in high-pressure units
- Coverage reliability across weekends and peak periods
These measures tell a fuller story than headcount alone ever will.
Why allied health and locum planning deserve more attention
Two areas are still underestimated in many hospital staffing conversations: allied health and physician coverage.
Allied health staffing affects far more than support functions. Imaging, respiratory, therapy, lab, and rehab roles have a direct impact on patient flow and care timelines. When those teams are understaffed, the entire delivery system feels it.
The same goes for locum tenens staffing. Many organizations still treat locums as a last-minute patch. In reality, it can be a smart part of a broader physician workforce strategy, especially during recruitment transitions, leave coverage, expansion periods, or specialty shortages.
Used well, flexible staffing does not weaken the workforce plan. It strengthens it.
The real goal is stability, not just coverage
The best workforce plans do not simply fill open shifts. They reduce chaos.
They give nurse leaders fewer last-minute surprises. They give HR a clearer hiring roadmap. They give finance a better handle on labor volatility. Most important, they give clinicians a better chance to do good work without carrying the weight of chronic understaffing.
That is the shift hospital leaders should be aiming for in 2026: from reactive staffing to workforce stability by design.
Final takeaway
Healthcare workforce planning is no longer optional for hospitals that want to protect access, control labor costs, and keep clinical teams from burning out.
The organizations that move first, forecast better, and build flexible staffing models will be in a stronger position than those still relying on last-minute fixes. Permanent hiring still matters. So do allied health staffing, travel talent, and locum tenens support. The advantage comes from knowing when and how to use each one.
For hospital leaders, the question is no longer whether workforce pressure is coming. It is whether the staffing strategy is strong enough to absorb it.
If your organization is rethinking coverage, retention, and workforce flexibility for the year ahead, this is the right time to build a plan that matches the reality on the floor.
Leave Your Comment Here